Health care for the elderly is from primary care, general hospital and geriatric unit.
Within these we will talk about the focus on specialized care.
These are units which caters exclusively to geriatric patients are divided into:
Medium-stay units. Restoring functional medical procedures, trauma or surgical.
Units for chronic patients or residences. Elderly with chronic deterioration of functional capacity, which can not be kept at home.
Geriatric day hospitals. Fragile patient care or nursing home.
Medium-stay units aim to get patients to recover some or all of your new business to perform activities of daily living.
The nurse in these units performs a function but also teaching assistance.
Numerous studies have observed improvements in patients who have gone through these units, such as: improved sleep, behavioral, drug reduction.
So it is important to establish the nursing care plan individualized, ongoing evaluation and development of interventions for both the patient and the family. Since it is very important to involve the family to assist in the recovery process of the patient.
These units must be used in a timely manner, because we can not get to the elderly is continually entering these, which is somewhat difficult for regular relapses in these patients. It is therefore important to make a good health education to the patient and caregiver.
"The health education addresses not only the transmission of information, but also the promotion of motivation, self-esteem and personal skills necessary to take action to improve health.'s Health education includes not only information on to the social, economic and environmental causes that influence health, but also referred to the risk factors and behaviors, and the use of the healthcare system. "
Health education is divided into: - Primary Prevention. - Secondary prevention. - Tertiary Prevention.
In the following video makes clear what would be a proper health education.
Speaking of 2020, indicating what would be the ideal model of prevention and promotion, especially in chronic patients.
I totally agree with this video, these would be the desired results and ideals, but in order to reach a realization that's needed. I think there is nothing that is impossible to get, just need our efforts and the fight for a healthy society and health.
As nurses have an important role in spreading this message, but anyone can help this simply with care and love your body a little more.
"An approach that improves the quality of life of patients and families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychological and spiritual "
We talk about terminal illness when: - There is an advanced disease, with a life expectancy of less than six months. - When no response to specific treatment. - When presented multiple symptoms that are continually changing and evolving for the worse.
You have any of these conditions: cancer, AIDS, Enf. Neuron, Renal Failure, Respiratory Failure, Heart Failure, Liver Failure, etc.
It is important to establish a trusting relationship with patients and family. Providing understanding, listening skills and emotional support.
The main nursing care are:
Control of pain. EVA Scale.
Keep calm and pleasant.
Maintenance of hygiene.
It should affect the mouth, cleaning mucus, saliva, change of clothes, diaper soaker.
Postural changes as pattern, usually every hour, but also according to the state in which the patient is located.
If the patient is conscious, never be supine, risk of aspiration.
Controlling the constants in turn.
Provide the wedge, bottle, if you can. Urination and defecation control.
Maintain body temperature, clothing. Decreases blood flow.
If you can take fluids help to take, but keep hydrated. Moisten lips occasionally.
It is important not to make inappropriate comments, since it is known that the last sense to be lost is the ear. Out of respect for the patient.
Providing pain medication is an irrevocable right of the patient, and that is does not have to suffer in this last stage.
Urinary incontinence is the involuntary loss of urine and objective, producing at the wrong time, in an amount problematic: hygienic, social, psychically, limiting.
To better understand this, see the following video of the ONI.
In all treatments, I focus on the consevador as it is the easiest and most common.
Kegel exercises:
Bladder training:
Establer is a pattern at the time of urination.
Biofeedback: Neuromuscular Therapy for information.
Vaginal cones:
They are used to fortalezer the pelvic floor.
Electrostrimulation:
It consists of applying electric shocks to exercise the pelvic floor and inhibit detrusor contractions. It is similar to Kegel exercises, but exogenously.
Bibliography:
1. Aguilar Navarro SG. Incontinencia urinaria en el adulto mayor. Rev Enferm Inst Mex Seguro Soc 2007; 15(1): 51-56
2. Robles J. La incontinencia urinaria. Anales Sis San Navarra. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1137-66272006000300006&lng=es
Constipation is a disturbance of intestinal transit, which is a decrease of stools, hard stools and painful bowel movements.
Constipation is considered to have fewer than three bowel movements per week.
According to the article Benito Key: "the elderly are among those most affected approximately 20% of noninstitutionalized older people have symptoms of constipation being 80% of those who suffer institutionalized, especially percentage increases with age. "
The variables that must be taken into account in assessing constipation are: - Frequency defecation. - Fecal weight. - Fecal consistency. - Effort defecation. - Satisfaction voidal.
The risk factors are:
Fluid intake.
Diet.
Mobility.
Environment.
Constipation medications.
Gastrointestinal obstruction.
Spinal cord dysfunction.
Pelvic floor dysfunction.
Irritable bowel syndrome.
Anxiety, depression, cognitive dysfunction.
The main complications of constipation are:
- Faecaloma.
- Anal fissure.
- Colonic ulcers.
- Risk of cancer.
- Cardiovascular complications.
Some easy steps to follow to prevent constipation are:
- Drink at least 1.5 of water a day as it moisturizes and increases intestinal motility.
- High-fiber diet, as it retains water.
- Establish a schedule of meals ordered, up to 6 a day.
- Eat slowly and chew well.
- Perform daily moderate exercise at least 30 minutes a day walking.
- Go to the bathroom quietly.
As a treatment, are laxatives. They are those that increase the intestinal bolus, the osmotic catárquicos stimulants, lubricants and rectal.
It is important to avoid excessive use of laxatives as they are harmful, irritating the bowel causing alterations. It is advisable to ask a specialist before using any drug.
Falls are a major cause of injury and death immobility in the elderly.
The elderly have a degeneration of the movements, have "run senile", noted for instability, short steps, stiffness, reduced oscillation of the arms.
It is known that the active ancianoes falls, although less common, have worse consequences.
With age and they lose some reflexes are slower.
WHO defines the fall as a result of any event which tumbles down the person against their will.
When an old man suffers a fall, are serious physical, psychological and social.
Bibliography:
1. González Sanchez RL. Rodríguez Fernández MM, Ferro Afonso MJ, García Milián JR. Caídas en el anciano. Consideraciones generales y prevención. Rev Cubana Med Gen Integr. Volumen 15 Nº1. 1999.
Alzheimer's is one of the most common diseases of dementia in the elderly.
This disease is caused by the loss of brain cells slowly, not currently know the cause of this loss of neurons and therefore no effective treatment is known.
This loss of memory is:
• Short term: forget what you just did, happen.
• Long term: memories disappear.
Symptoms of dementia:
• Inability to learn new things.
• Recall information from the past.
• Inability to speak and express themselves clearly.
• Problems recognizing objects.
• Change in personality.
• In some cases they have problems to work and perform morning activities like showering.
• Many times there are cases of depression or anxiety.
• In extreme situations the patient does not remember anything of this, but remember what you did ten years ago. (You remember the past more than the present).
Is one of the diseases that affects people around 65 years old, has no effective treatment
and it is irreversible.
It is estimated that dementia doubles every five years from the coming 65years and to affect 30% of patients older than 85 years.
The loss of function is very slow and there are very long courses (over 15 years), can be divided into:
- First stage:From one to three years.
- Second stage:Two to ten years.
- Third stage: Eight to twelve years.
People with dementia require more patience, support and understanding. It is a difficult situation in which nurses have to care for both the patient and the family as the primary caregiver usually has a significant emotional distress.
I leave here a video of World Alzheimer's Day 2012, in which some people tell their experiences. Hope you like it! I really found very moving and helpful to get in the position of the other person and understand from near this disease.








.jpg) They are used to fortalezer the pelvic floor.
They are used to fortalezer the pelvic floor.  Constipation is a disturbance of intestinal transit, which is a decrease of stools, hard stools and painful bowel movements.
Constipation is a disturbance of intestinal transit, which is a decrease of stools, hard stools and painful bowel movements.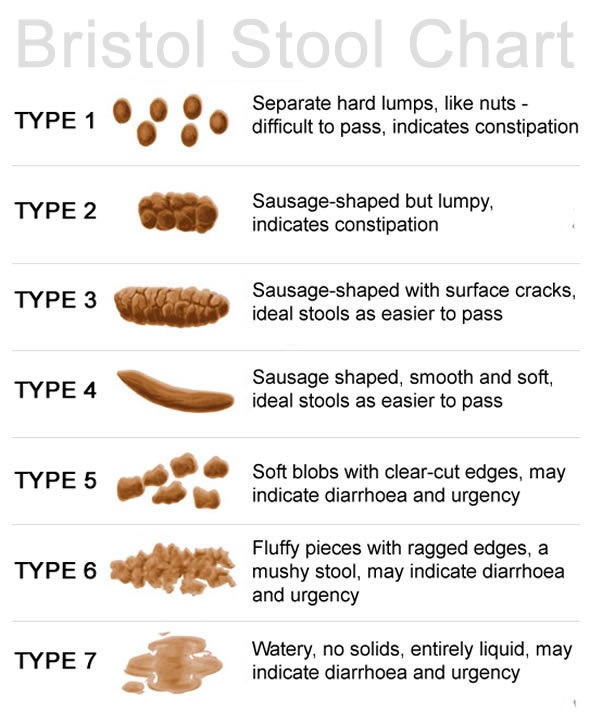
 Falls are a major cause of injury and death immobility in the elderly.
Falls are a major cause of injury and death immobility in the elderly. Alzheimer's is one of the most common diseases of dementia in the elderly.
Alzheimer's is one of the most common diseases of dementia in the elderly.
 The loss of function is very slow and there are very long courses (over 15 years), can be divided into:
The loss of function is very slow and there are very long courses (over 15 years), can be divided into: