I leave a video for you to consider.
And this one to put a smile on your face.
Thanks for reading my blog!! =)








.jpg) They are used to fortalezer the pelvic floor.
They are used to fortalezer the pelvic floor.  Constipation is a disturbance of intestinal transit, which is a decrease of stools, hard stools and painful bowel movements.
Constipation is a disturbance of intestinal transit, which is a decrease of stools, hard stools and painful bowel movements.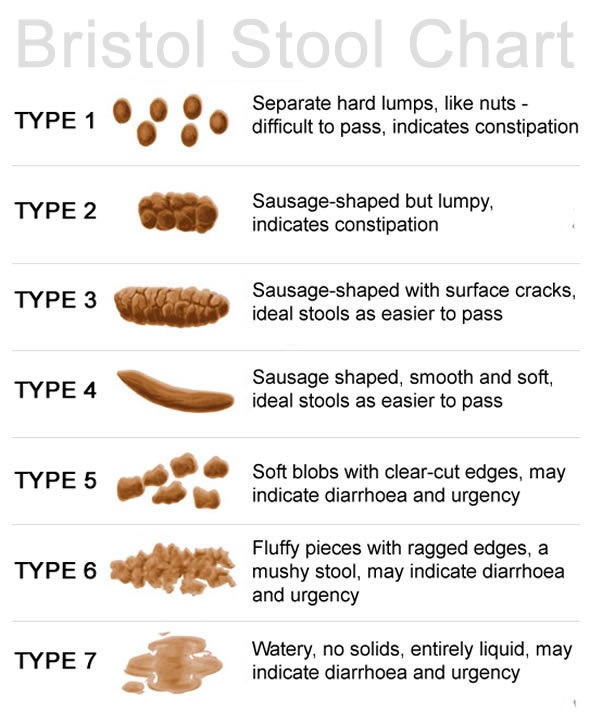
 Falls are a major cause of injury and death immobility in the elderly.
Falls are a major cause of injury and death immobility in the elderly. Alzheimer's is one of the most common diseases of dementia in the elderly.
Alzheimer's is one of the most common diseases of dementia in the elderly.
 The loss of function is very slow and there are very long courses (over 15 years), can be divided into:
The loss of function is very slow and there are very long courses (over 15 years), can be divided into: The immobility is the decreased ability to perform activities of daily living impairment of motor functions.
The immobility is the decreased ability to perform activities of daily living impairment of motor functions.





 According to the study by Gago et all, maceration is the most common problem when using dressings based on moist wound healing. Occurs when the exudate is poorly controlled, which saturates the surrounding skin and cause pain, slowing the evolution of the wound, increasing its size.
According to the study by Gago et all, maceration is the most common problem when using dressings based on moist wound healing. Occurs when the exudate is poorly controlled, which saturates the surrounding skin and cause pain, slowing the evolution of the wound, increasing its size.


